Author Information1
Li, J.2; Liu, T.3; Nokta, N.4; Shah, A.5; Suri, R.6; Wang, A.7
(Editor: Inoue, M.8)
1 All authors are listed in alphabetical order.
2 Tesoro High School, CA, 3 Gretchen Whitney High School, CA, 4 King Abdallah Academy, VA, 5 Langley High School, VA, 6 Flint Hill Private High School, VA, 7 Torrey Pines High School, CA
8 George Mason University
Background: Multiple studies have investigated the factors influencing the completion of Advance Care Planning (ACP) in the United States of America [1][2]. ACP involves preparing and discussing future medical care when the patient is incapacitated in some way so that they retain some autonomy of their decisions even when they are unable to communicate effectively [3][4]. Previous studies have compared rural and urban nursing home residents and found that rural nursing home residents were more likely to have advance directives in place and less likely to experience extended hospitalizations or intensive care stays compared to their urban counterparts [5]. Between urban and rural patients with Physician Orders for Life-Sustaining Treatment forms, orders for full treatment are less prevalent among rural patients, with a preference towards DNR and limited intervention [6]. However, the findings on rural vs. urban are not consistent. Another line of research has examined racial disparities, revealing that White/non-Hispanic residents were over twice as likely as Black residents to have documented advance directives, with county-facility characteristics accounting for a significant portion of this difference. Additionally, regional variations in Medicare spending have been linked to higher rates of ACP engagement [7][8]. Positive interactions, emotional support, and encouragement from family members play significant roles in motivating patients to undertake ACP [2][9] leading to more appropriate care during their end-of-life phase. Conversely, strained relationships characterized by criticism or lack of support may discourage individuals from engaging in ACP.
Objective: The objective of this study was to determine the influence of geographical and familial factors on advance directive (AD) engagement in the United States.
Methods: The project dataset contains 10,113 respondents (2002-2019) from the US Census Bureau and Health and Retirement Study, prepared by our faculty advisors at George Mason University. This dataset includes information on marriage status, census regions and family structure. All the analysis was conducted and visualized using QGIS.
Results: Individuals residing in urban locations are more likely to apply and use ADs and have end-of-life instructional measures arranged for themselves. This can be explained by people in urban areas having an increased access to hospitals and healthcare information and innovation compared to those in rural areas. A correlation can be made to map models – the east coast of the United States is more densely populated compared to rural areas in the midwest. In terms of the family structure, married individuals and individuals with children are more likely to engage in ADs. Additionally, spouses and children are more likely to be main decision makers for medical treatment, indicating the important role of family members in decision-making when patients have not explicitly communicated their end-of-life preferences.
Figure 1. Percentage of people with living will by location
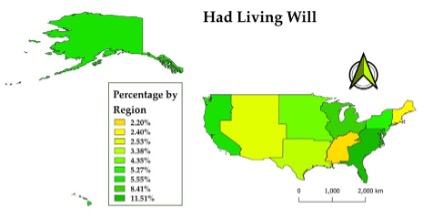
Fig 2: Percentage of people married or partnered
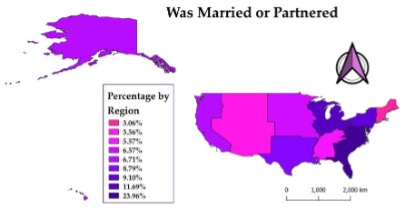
Conclusions: The study found that individuals living in urban areas on the East Coast are more likely to engage in ADs than individuals living in rural areas in the U.S. Additionally, married individuals and individuals with children are more likely to engage in ADs. When individuals are married and have children, they are more likely to appoint their adult children as designated healthcare decision makers than their spouses.
References
- Bischoff, K. E., Sudore, R., Miao, Y., Boscardin, W. J. & Smith, A. K. (2013). Advance Care Planning and the Quality of End-of-Life Care among Older Adults. Journal of the American Geriatrics Society, 61(2), 209-214. https://doi.org/10.1111/jgs.12105
- Fried, T.R., Redding, C.A., Robbins, M.L., O’Leary, J.R. & Iannone, L. (2011). Agreement between Older Persons and their Surrogate Decision Makers Regarding Participation in Advance Care Planning. Journal of the American Geriatrics Society, 59(6), 1105-1109. https://doi.org/10.1111/j.1532-5415.2011.03412.x
- Moorman, S.M. & Inoue, M. (2013). Persistent Problems in End-of-Life Planning Among Young- and Middle-Aged American Couples. The Journals of Gerontology: Series B, 68(1), 97-106. https://doi:10.1093/geronb/gbs103
- Carr, D., Luth, E.A., Massey, D.S. & Cook, K.S. (2019). Well-Being at the End of Life. Annual Review of Sociology, 45(1), 515-534. https://doi.org/10.1146/annurev-soc-073018-022524
- Elliot, V., Morgan, D., Kosteniuk, J., Bayly, M., Froehlich Chow, A., Cammer, A., O’Connell, M.E. & Ginsberg, S.D. (2021). Palliative and end-of-life care for people living with dementia in rural areas: A scoping review. PLoS One, 16(1), e0244976. https://doi.org/10.1371/journal.pone.0244976
- Schmidt, T.A., Zive, D., Fromme, E.K., Cook, J.N.B. & Tolle, S.W. (2014). Physician Orders for Life-Sustaining Treatment (POLST): Lessons learned from analysis of the Oregon POLST Registry. Resuscitation, 85(4), 480–485. https://doi.org/10.1016/j.resuscitation.2013.11.027
- Rao, J.K., Anderson, L.A., Lin, F.-C. & Laux, J. P. (2014). Completion of Advance Directives Among U.S. Consumers. American Journal of Preventive Medicine, 46(1), 65-70. https://doi.org/10.1016/j.amepre.2013.09.008
- Nicholas, L. H., Langa, K.M., Iwashyna, T.J. & Weir, D.R. (2011). Regional Variation in the Association Between Advance Directives and End-of-Life Medicare Expenditures. JAMA, 306(13), 1447-1453. https://doi.org/10.1001/jama.2011.1410
- Boerner, K., Carr, D. & Moorman, S. (2013). Family Relationships and Advance Care Planning: Do Supportive and Critical Relations Encourage or Hinder Planning? The Journals of Gerontology: Series B, 68(2), 246-256. https://doi.org/10.1093/geronb/gbs161