Racial & Sex Disparities in Lupus & Transplant Outcomes
Author Information1
Endlaw, Shriya2; Farhan, Hamza3.; Li, Jason4; Peng, Candice5; Skaggs, Sarah3; Tan, Alexander6
(Editor: Koizumi, Naoru7)
1 All authors are listed in alphabetical order.
2 Chantilly High School, VA, 3George C. Marshall High School, VA, 4Thomas S. Wootton High School, CA, 5Tesoro High School, CA, 6San Mateo High School, CA,
7George Mason University, VA
Background: Systemic lupus erythematosus (SLE) is an autoimmune disease with both high morbidity and mortality rates [1]. Clinical symptoms, laboratory findings, and optional biopsy results are the basis for early diagnosis of SLE. The disease is well-known for its butterfly rash that appears mainly on women at child bearing ages, and patients should be treated with antimalarials with hydroxychloroquine presenting the best results; it has a higher rate of remission, fewer relapses and reduced damage in the course of the disease [2]. Although there has been significant progress made in regards to SLE, the number of SLE patients who face End Stage Renal Disease (ESRD) has increased from 1.6 to 4.9 million from 1982 to 2004 [3]. Patients with ESRD were tested to predict a 3-year allograft survival after transplantation. Graft has an 84% chance of 3-year survival if the patient didn’t need dialysis during the first week compared to 58% if dialysis was needed during the first post transplantation week. For those who had needed dialysis for the first week, if their maintenance immunosuppressive regimen contained prednisone, took hemodialysis, and was older than 50 years, their graft had a lower probability of survival [1]. Adding on, much advancement and findings regarding SLE has led to the discovery of correlation between the disease and minority populations. The Centers for Disease Control and Prevention National Lupus Registries found that people of color (African Americans, APIs, and Hispanics) are more susceptible to SLE. Studies show that psychosocial stressors are potential exacerbators of SLE which can activate the inflammatory pathways. Often exposed to racial discrimination, people of color experience a large source of stress which can cause many health disparities, which in turn, can lead to the further worsening of SLE [4]. It has also been studied that after a kidney transplant, many patients have gotten rid of their Lupus while others, specifically African Americans (AA) have gotten Lupus back with other symptoms [3]. Adding on, five years after a kidney transplant for Lupus Nephritis (LN) graft survival for AF is at 63%, while for non-AA the graft survival rate is at 78.3%. Further, AA of lower median household income (MHI) are more likely to experience quicker graft loss compared to AA of higher MHI. For non-AA, there was no significant trend between MHI and graft loss [5]. While LN significantly increased the risk of graft failure, rejection remained the primary driver of graft failure incidence. These results emphasized that these findings should not discourage patients with Lupus from considering a kidney transplant [6].
Objective: The study investigated how the outcomes of kidney transplants differ by sex and race in the transplant recipients with SLE diagnosis.
Methods: A retrospective analysis was performed using the UNOS database between January 1, 2010 and June 30, 2022. The basic patient, donor and transplant characteristics were compared by recipient sex and ethnicity using T- and Chi-sq. tests. Survival curves and the estimates for transplant outcomes by sex and ethnicity were obtained using the Kaplan-Meier (KM) Product Limit method. In the analysis, patient death and graft failure were the end-points. Patients who did not experience any of the end-points or whose life and graft status was unknown were censored on the last follow-up or the last day of the study. Log-rank tests were used to test the equality of the curves. All analyses were done in R and the statistical significance was defined by p<0.05.
Results: Overall, male patients were more likely to experience the graft failure. African American patients were also more likely to experience the graft failure (p<0.001) while Asians and Hispanic patients were less likely to experience the graft failure (p<0.001).
Table 1. Descriptive Statistics
| Patient Sex and Ethnicity | No Graft Failure (n = 3300) | Graft Failure (n = 837) | p-value |
| Male, n (%) | 552 (16.73%) | 172 (20.55%) | 0.011 |
| White | 559 (16.94%) | 166 (19.83%) | 0.554 |
| African American | 1614 (48.91%) | 474 (56.63%) | < 0.001 |
| Hispanic | 785 (23.79%) | 143 (17.08%) | < 0.001 |
| Asian | 276 (8.36%) | 41 (4.10%) | < 0.001 |
| Other | 66 (2%) | 13 (1.55%) | 0.483 |
Figure 1. Kaplan Meier Survival Curves for Graft Failure
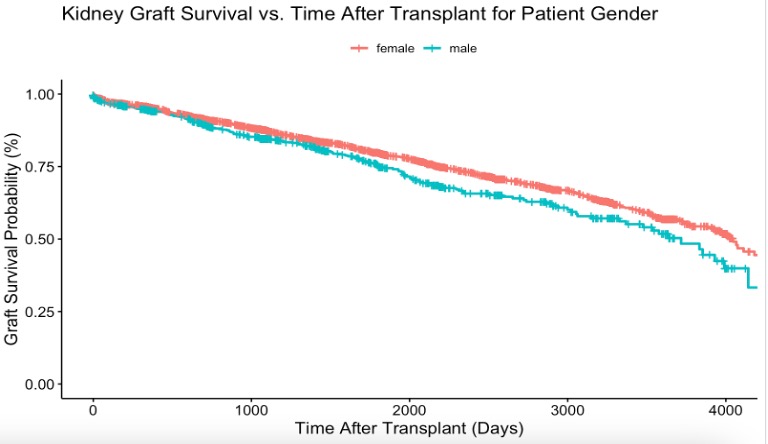
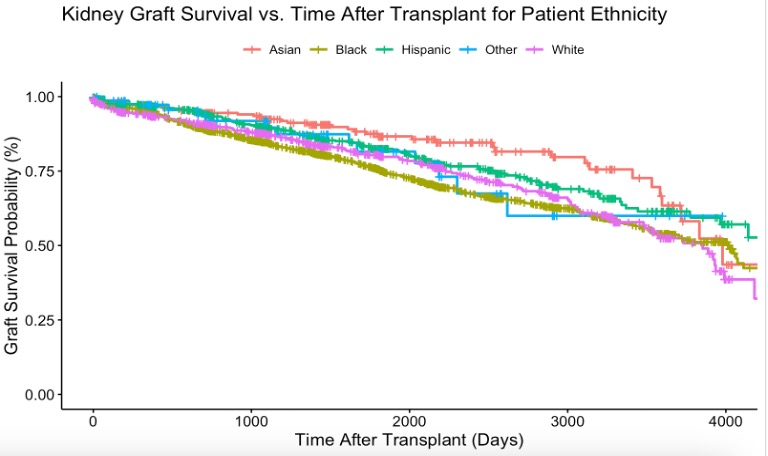
Conclusions: Male and African American patients are at higher risk for graft failure among the kidney transplant recipients whose primary diagnosis was SLE.
References
- Tang, H., Poynton, M.R., Hurdle, J.F., Baird, B.C., Koford, J.K. and Goldfarb-Rumyantzev, A.S., 2011. Predicting three-year kidney graft survival in recipients with systemic lupus erythematosus. Asaio Journal, 57(4), pp.300-309. doi: 10.1097/MAT.0b013e318222db30
- Kuhn, A., Bonsmann, G., Anders, H.J., Herzer, P., Tenbrock, K. and Schneider, M., 2015. The diagnosis and treatment of systemic lupus erythematosus. Deutsches Ärzteblatt International, 112(25), p.423. doi: 10.3238/arztebl.2015.0423
- Lionaki, S., Skalioti, C. and Boletis, J.N., 2014. Kidney transplantation in patients with systemic lupus erythematosus. World Journal of Transplantation, 4(3), p.176. doi:10.5500/wjt.v4.i3.176
- Drenkard, C. and Lim, S.S., 2019. Update on lupus epidemiology: advancing health disparities research through the study of minority populations. Current opinion in rheumatology, 31(6), p.689. doi:10.1097/BOR.0000000000000646
- Nee, R., Jindal, R.M., Little, D., Ramsey-Goldman, R., Agodoa, L., Hurst, F.P. and Abbott, K.C., 2013. Racial differences and income disparities are associated with poor outcomes in kidney transplant recipients with lupus nephritis. Transplantation, 95(12), pp.1471-1478. doi:10.1097/TP.0b013e318292520e
- Contreras, G., Mattiazzi, A., Guerra, G., Ortega, L.M., Tozman, E.C., Li, H., Tamariz, L., Carvalho, C., Kupin, W., Ladino, M. and LeClercq, B., 2010. Recurrence of lupus nephritis after kidney transplantation. Journal of the American Society of Nephrology: JASN, 21(7), p.1200. www.ncbi.nlm.nih.gov/pmc/articles/PMC3152228/.
Optimal Immunosuppressive Regimen for Pediatric Liver Transplant Recipients
Author Information1
Ashok, Keshav2; Gottumukkala, Ananya3; Panesar, Meher4; Song, Jessika (Jiayao)5; Yang, Roy6.
(Editor: Koizumi, Naoru7)
1 All authors are listed in alphabetical order
2 Westview High School, OR, 3 Thomas Jefferson High School for Science and Technology, VA,
4 Westfield High School, VA, 5 University of British Columbia, Canada, 6 Winston Churchill High School, MD, 7 George Mason University, VA
Background: The main obstacle to success is transplant rejection and managing the side effects of immunosuppressive medications. Induction and maintenance types of immunosuppressive medications are used in transplants. Induction therapy is used temporarily, only immediately following transplantation while maintenance immunosuppressive drugs are started and given long-term. Maintenance therapy can involve the use of antibodies or higher doses of medications. The standard triple medication regimen usually consists of the combination of a calcineurin inhibitor, an antiproliferative agent and a corticosteroid. These have been found to be more effective in balancing the risks of suppressed immune system with the benefit of organ transplant. However, the immunological risks (driven by age, preconditions, and other factors) of the child/pediatric patient should be considered, and the immunosuppressive therapy should be followed by therapeutic drug monitoring. [1]
A study conducted by Feng, Ekong & Lobritto (2012) reported that immunosuppression came with many toxic effects. Some of these include renal dysfunction, infection, metabolic perturbation, and malignancy [2]. To add on, Blondet, Healy & Hsu (2017) reported that the 2 most common immunosuppressants, tacrolimus and cyclosporine, were both known to have long-term side effects in children, which included nephrotoxicity, neurotoxicity, infection, and malignancy. Patient survival rates for pediatric liver transplant recipients after the use of immunosuppressive agents were 94% after one year, 91% after five years, and 88% after 10 years [3]. They also found that the side effects of immunosuppressive medications were severe in pediatric liver transplant recipients. Some immunosuppressive agents, such as tacrolimus, antithymocyte globulin, basiliximab, and others, might cause side effects including sensitivity, nausea, vomiting, diarrhea, high blood pressure, acne, abdominal pain, discomfort, mood swings and more. While immunosuppressants help with preventing rejection, it may be a challenge for pediatric patients since their reactions to the medications may be critical.
Objective: The study investigated how transplant outcomes (graft failure and patient mortality) vary by induction immunosuppressive therapy among pediatric liver transplant recipients.
Methods: A retrospective analysis was performed using the UNOS database between January 1, 2010 and June 30, 2022. The basic patient, donor and transplant characteristics were compared by basic demographics (age, sex and ethnicity) as well as induction and maintenance immunosuppressive therapies using T- and Chi-sq. tests. Survival curves and the estimates for transplant outcomes by induction and maintenance therapies were obtained using the Kaplan-Meier (KM) Product Limit method. In the analysis, patient death and graft failure were the end-points. Patients who did not experience any of the end-points or whose life and graft status was unknown were censored on the last follow-up or the last day of the study. Log-rank tests were used to test the equality of the curves. All analyses were done in R and the statistical significance was defined by p<0.05.
Results: There was a statistically significant difference in age between the group with graft failure (56.3) and the group without graft failure (54.5) (p < 0.001). Male patients were also more likely to experience graft failure. African American patients were more likely to experience graft failure, while Asian patients were less likely to experience graft failure (p < 0.001).
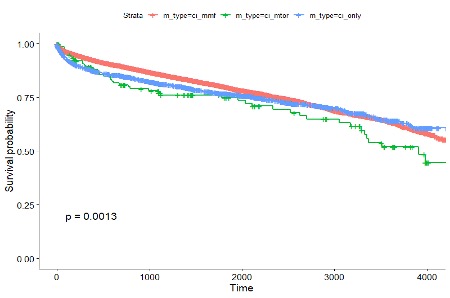
For the induction therapy, pediatric patients receiving Alemtuzumab (Campath) were much less likely to experience graft failure compared to other (antithymocyte globulin, basiliximab, and daclizumab) induction drugs (Figure 1: Panel A, p<0.001). Patient mortality survivals were similar, demonstrating that Alemtuzumab (Campath) reduces the patient mortality rate (Figure 1: Panel B, p<0.001).
Figure 1. Kaplan Meier Survival Curves by Induction Therapies

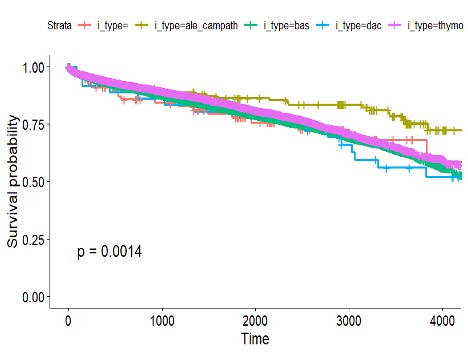
Panel A: Graft Survival Curves
Panel B: Patient Survival Curves
Figure 2. Kaplan Meier Survival Curves by Maintenance Therapy

Panel A: Graft Survival Curves
Panel B: Patient Survival Curves
Figure 3. Kaplan Meier Survival Curves by Steroid Use
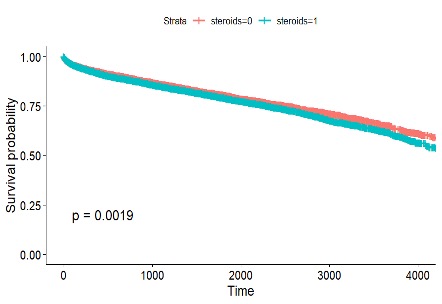
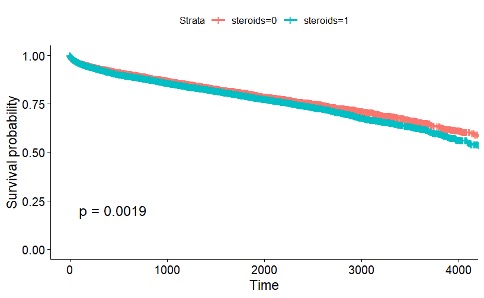
Panel A: Graft Survival Curves
Panel B: Patient Survival Curves
Conclusions: Pediatric liver transplant recipients who received alemtuzumab as the induction therapy had the best transplant outcomes while those recipients who received calcineurin inhibitors (tacrolimus or cyclosporine) with mammalian target of rapamycin (mTOR) as the maintenance therapy experienced the worst outcomes. Steroid use also worsened the outcomes.
References
- Lockridge, J. and Olyaei, A., 2019. Kidney Transplant-Immunosuppression and Rejection. Kidney Transplant Management: A Guide to Evaluation and Comorbidities, pp.29-42. https://link.springer.com/chapter/10.1007/978-3-030-00132-2_4
- Feng, S., Ekong, U.D., Lobritto, S.J., Demetris, A.J., Roberts, J.P., Rosenthal, P., Alonso, E.M., Philogene, M.C., Ikle, D., Poole, K.M. and Bridges, N.D., 2012. Complete immunosuppression withdrawal and subsequent allograft function among pediatric recipients of parental living donor liver transplants. Jama, 307(3), pp.283-293.
- Blondet, N.M., Healey, P.J. and Hsu, E., 2017, August. Immunosuppression in the pediatric transplant recipient. In Seminars in pediatric surgery (Vol. 26, No. 4, pp. 193-198). WB Saunders.
Geographical and Familial Factors in Engagement of Advance Directives
Author Information1
Li, Jessie2; Liu, Tyler3; Nokta, Nyla4; Shah, Ahaan5; Suri, Rohan6; Wang, Arthur7
(Editor: Inoue, Megumi8)
1 All authors are listed in alphabetical order.
2 Tesoro High School, CA, 3 Gretchen Whitney High School, CA, 4 King Abdallah Academy, VA, 5 Langley High School, VA, 6 Flint Hill Private High School, VA, 7 Torrey Pines High School, CA
8 George Mason University
Background: Multiple studies have investigated the factors influencing the completion of Advance Care Planning (ACP) in the United States of America [1][2]. ACP involves preparing and discussing future medical care when the patient is incapacitated in some way so that they retain some autonomy of their decisions even when they are unable to communicate effectively [3][4]. Previous studies have compared rural and urban nursing home residents and found that rural nursing home residents were more likely to have advance directives in place and less likely to experience extended hospitalizations or intensive care stays compared to their urban counterparts [5]. Between urban and rural patients with Physician Orders for Life-Sustaining Treatment forms, orders for full treatment are less prevalent among rural patients, with a preference towards DNR and limited intervention [6]. However, the findings on rural vs. urban are not consistent. Another line of research has examined racial disparities, revealing that White/non-Hispanic residents were over twice as likely as Black residents to have documented advance directives, with county-facility characteristics accounting for a significant portion of this difference. Additionally, regional variations in Medicare spending have been linked to higher rates of ACP engagement [7][8]. Positive interactions, emotional support, and encouragement from family members play significant roles in motivating patients to undertake ACP [2][9] leading to more appropriate care during their end-of-life phase. Conversely, strained relationships characterized by criticism or lack of support may discourage individuals from engaging in ACP.
Objective: The objective of this study was to determine the influence of geographical and familial factors on advance directive (AD) engagement in the United States.
Methods: The project dataset contains 10,113 respondents (2002-2019) from the US Census Bureau and Health and Retirement Study, prepared by our faculty advisors at George Mason University. This dataset includes information on marriage status, census regions and family structure. All the analysis was conducted and visualized using QGIS.
Results: Individuals residing in urban locations are more likely to apply and use ADs and have end-of-life instructional measures arranged for themselves. This can be explained by people in urban areas having an increased access to hospitals and healthcare information and innovation compared to those in rural areas. A correlation can be made to map models – the east coast of the United States is more densely populated compared to rural areas in the midwest. In terms of the family structure, married individuals and individuals with children are more likely to engage in ADs. Additionally, spouses and children are more likely to be main decision makers for medical treatment, indicating the important role of family members in decision-making when patients have not explicitly communicated their end-of-life preferences.
Figure 1. Percentage of people with living will by location
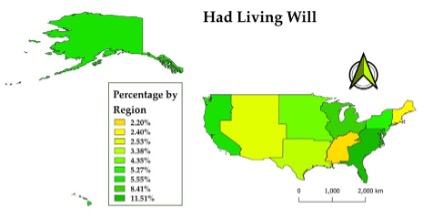
Fig 2: Percentage of people married or partnered
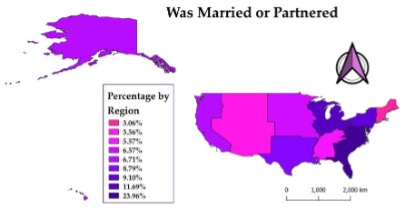
Conclusions: The study found that individuals living in urban areas on the East Coast are more likely to engage in ADs than individuals living in rural areas in the U.S. Additionally, married individuals and individuals with children are more likely to engage in ADs. When individuals are married and have children, they are more likely to appoint their adult children as designated healthcare decision makers than their spouses.
References
- Bischoff, K. E., Sudore, R., Miao, Y., Boscardin, W. J. & Smith, A. K. (2013). Advance Care Planning and the Quality of End-of-Life Care among Older Adults. Journal of the American Geriatrics Society, 61(2), 209-214. https://doi.org/10.1111/jgs.12105
- Fried, T.R., Redding, C.A., Robbins, M.L., O’Leary, J.R. & Iannone, L. (2011). Agreement between Older Persons and their Surrogate Decision Makers Regarding Participation in Advance Care Planning. Journal of the American Geriatrics Society, 59(6), 1105-1109. https://doi.org/10.1111/j.1532-5415.2011.03412.x
- Moorman, S.M. & Inoue, M. (2013). Persistent Problems in End-of-Life Planning Among Young- and Middle-Aged American Couples. The Journals of Gerontology: Series B, 68(1), 97-106. https://doi:10.1093/geronb/gbs103
- Carr, D., Luth, E.A., Massey, D.S. & Cook, K.S. (2019). Well-Being at the End of Life. Annual Review of Sociology, 45(1), 515-534. https://doi.org/10.1146/annurev-soc-073018-022524
- Elliot, V., Morgan, D., Kosteniuk, J., Bayly, M., Froehlich Chow, A., Cammer, A., O’Connell, M.E. & Ginsberg, S.D. (2021). Palliative and end-of-life care for people living with dementia in rural areas: A scoping review. PLoS One, 16(1), e0244976. https://doi.org/10.1371/journal.pone.0244976
- Schmidt, T.A., Zive, D., Fromme, E.K., Cook, J.N.B. & Tolle, S.W. (2014). Physician Orders for Life-Sustaining Treatment (POLST): Lessons learned from analysis of the Oregon POLST Registry. Resuscitation, 85(4), 480–485. https://doi.org/10.1016/j.resuscitation.2013.11.027
- Rao, J.K., Anderson, L.A., Lin, F.-C. & Laux, J. P. (2014). Completion of Advance Directives Among U.S. Consumers. American Journal of Preventive Medicine, 46(1), 65-70. https://doi.org/10.1016/j.amepre.2013.09.008
- Nicholas, L. H., Langa, K.M., Iwashyna, T.J. & Weir, D.R. (2011). Regional Variation in the Association Between Advance Directives and End-of-Life Medicare Expenditures. JAMA, 306(13), 1447-1453. https://doi.org/10.1001/jama.2011.1410
- Boerner, K., Carr, D. & Moorman, S. (2013). Family Relationships and Advance Care Planning: Do Supportive and Critical Relations Encourage or Hinder Planning? The Journals of Gerontology: Series B, 68(2), 246-256. https://doi.org/10.1093/geronb/gbs161
Gut Microbiome and Kidney Transplant
Author Information1Cho, Minseo2; Herdrich, Kyle3; Jung, Isaac4; Liu, Jiahui5; Wang, Jason (Xinxiang)4; Yang, Jonathan6
(Editor: Li, Meng-Hao7)
1 All authors are listed in alphabetical order.
2 Episcopal High School, VA, 3 Troy High School, CA, 4 Flintridge Preparatory School, CA, 5 Mission San Jose High School, CA, 6 The Lawrenceville School, CA
7 George Mason University, VA
Background: The gut microbiota, comprising the entire population of microorganisms that colonize the colon, has evolved over time to establish a symbiotic relationship with the human body, yielding mutual benefits [1]. This microbiome plays a pivotal role in critical bodily functions, including biosynthesis, short-chain fatty acid (SCFA) production, gut regulation, and immune system function. Under normal circumstances, these gut bacteria are referred to as indigenous microbiota, performing their customary functions; however, in the presence of disturbances, detrimental or opportunistic bacteria emerge, known as pathobionts [2]. Imbalances within the gut microbiota have been associated with various diseases, including obesity, metabolic disorders, inflammatory bowel diseases, colorectal cancer, allergies, and autoimmune disorders [1]. Of particular concern is the impact of immunosuppressants and antibiotics administered after kidney transplant surgeries, as they disrupt the patients’ gut microbiome, alter indigenous microbiota, and promote the proliferation of pathobionts, resulting in a condition known as dysbiosis. Dysbiosis, in turn, may facilitate the development of acute kidney injury (AKI) by modifying SCFA composition and generating elevated levels of toxins. Both AKI and pathobionts can contribute to the progression of atherosclerosis, cardiovascular diseases, inflammation, and chronic kidney disease (CKD). If left untreated, CKD can escalate to infections and even rejection of the newly transplanted kidney by the recipient’s immune system [2].
Objective: This project aims to 1) examine the degree of change occurred in the abundance and diversity of the gut microbiome, before and after kidney transplantation, and 2) identify treatments that support the microbiome in returning to its healthy, stable state.
Methods: The project dataset comprises data from 10 kidney transplant patients at the University of Toledo Medical Center, provided by our GMU faculty advisors. This dataset includes information on the gut microbiome species before and after transplantation for each patient. To analyze the patient data, we employed a t-test to identify microbiota species that exhibited significant changes in absolute abundance before and after transplantation. Furthermore, we utilized Pearson correlation analysis to identify microbiota species that displayed significant interactions before and after transplantation. Finally, we demonstrated that species with both significant changes in absolute abundance and significant interactions before and after transplantation. All statistical analyses were conducted using the R program, provided by our GMU faculty advisors.
Results: Out of the 141 microbiota species, only 5 exhibited significant changes in their absolute abundance, pre and post kidney transplantation. Phocaeicola contributes to colon health by breaking down complex heteropolysaccharides to SCFA [3]. Clostridium and Hungatella are harmful species that can cause diarrhea and inflammation in the gut [4]. Hungatella is associated with severe diseases such as septicemia (Juárez et al., 2021). Members of the Firmicutes species produce butyrate, an anti-inflammatory agent [5]. A decrease of this species suggests a decline in gut health and microbiome diversity. Streptococcus thermophilus is an important modulator of uremic toxins in the gut of patients diagnosed with chronic kidney disease [6]. In addition, our data analysis identified 78 species pairs with significant correlations. Of the 78 pairs, only 9 pairs (Hungatella and Clostridium) are shown here because they exhibited high correlations AND significant changes in absolute abundance pre- and post-transplantation.
Table 1. Species with Significant Change in Abundance
| Genus | Mean Difference | P-value |
| Phocaeicola | 15219.09 | 0.035 |
| Hungatella | 1134.68 | 0.062 |
| Clostridium | 8279.27 | 0.09 |
| Firmicutes_u_g | -13113.33 | 0.033 |
| Streptococcus | 2704.62 | 0.095 |
Table 2. Species with Significant Interactions
| Genus 1 | Genus 2 | Pearson Correlation Coefficient | P-value |
| Hungatella | Intestinimonas | -0.79 | 0.007 |
| Hungatella | Coprobacillus | 0.85 | 0.002 |
| Hungatella | Erysipelatoclostridium | 0.97 | <0.001 |
| Clostridium | Faecalibacterium | 0.77 | 0.009 |
| Clostridium | Oscillibacter | 0.81 | 0.004 |
| Clostridium | Flavonifractor | 0.83 | 0.003 |
| Clostridium | Dysosmobacter | 0.8 | 0.005 |
| Clostridium | Clostridia_u_g | 0.78 | 0.008 |
| Clostridium | Lachnospiraceae_u_g | 0.79 | 0.007 |
Figure 1: Microbial Network Change After Kidney Transplant
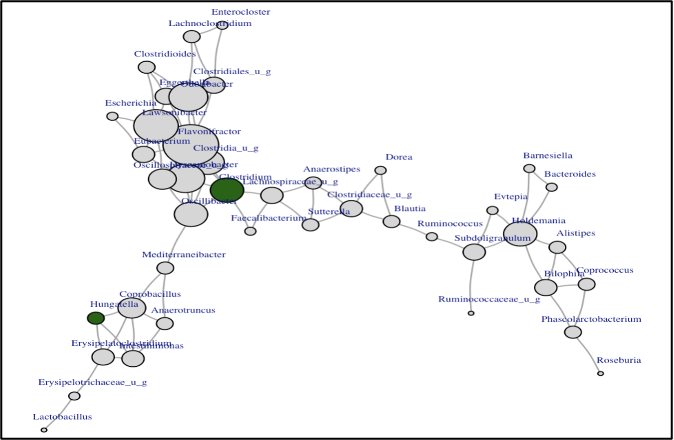
Conclusions: Through patient data analysis and literature research, this project identified the most impactful bacteria that could play a key role in restoration of patients’ gut microbiome diversity, richness, and overall health.
References
- Jandhyala, S.M., Talukdar, R., Subramanyam, C., Vuyyuru, H., Sasikala, M. and Reddy, D.N., 2015. Role of the normal gut microbiota. World journal of gastroenterology: WJG, 21(29), p.8787.
- Salvadori, M., 2021. The Microbiota and Kidney Transplantation: Influence on the Graft. Urology, 9, pp.95-105.
- Lück, R. and Deppenmeier, U., 2022. Genetic tools for the redirection of the central carbon flow towards the production of lactate in the human gut bacterium Phocaeicola (Bacteroides) vulgatus. Applied Microbiology and Biotechnology, 106(3), pp.1211-1225.
- Mayo Clinic. (2021, August 27). C. difficile infection. Mayo Clinic. https://www.mayoclinic.org/diseases-conditions/c-difficile/symptoms-causes/syc-20351691.
- Edermaniger, L. (2021, June 21). Firmicutes bacteria: What are they and why are they important? Atlas Biomed blog | Take control of your health with no-nonsense news on lifestyle,
- Gut microbes and genetics. https://atlasbiomed.com/blog/guide-to-firmicutes/
- Vitetta, L., Chen, J. and Clarke, S., 2019. The vermiform appendix: an immunological organ sustaining a microbiome inoculum. Clinical Science, 133(1), pp.1-8.
Regional and Seasonal Variation of Cyanotoxins
Author Information1
Aaravabhoomi, Hasika2; Field, Daniel3; Gibson, Adam4; Kou, Sissy5; Schlueter, Matthew6; Shah, Rohan7
(Editor: Baxt, Patrick Raymond8)
1 All authors are listed in alphabetical order.
2 McLean High School, VA, 3 Los Altos High School, CA, 4 Yorktown High School, VA, 5 Cupertino High School, CA, 6 James Madison School, VA, 7 Poolesville High School, CA
8 George Mason University
Background: Harmful Algal Blooms (HABs) and their toxins thrive in warm, nutrient-rich freshwater conditions, and can produce harmful cyanotoxins. Typically, these cyanotoxins take the form of hepatotoxins, dermatoxins, or neurotoxins. Exposure to cyanotoxins can occur in various fashions, including skin-to-water contact, inhalation of fumes, ingestion of contaminated water, and indirect ingestion through contaminated water sources or aquatic animals [1]. Exposure to microcystins, a common hepatotoxin found in cyanobacteria blooms, has been linked to fatal liver damage in both humans and dogs [3]. Additional evidence connects cyanotoxin BMAA to neurodegenerative diseases, such as ALS and Parkinson’s disease [5]. Minimal treatment options are widely available. Government bodies therefore focus their efforts on cyanobacterial toxicosis prevention, commonly issuing public safety alerts and advisory warnings around peak HAB exposure areas [3].
Objective: This research examines how HAB blooms and cyanobacteria outbreaks vary both regionally and seasonally across the United States from 2008-2018.
Methods: A series of t-tests, chi-squared tests, and ANOVA specifications stratified by region and season underlie the reported results. Each utilizes the US EPA Cyanobacteria state reported events and recreation advisories data from 2008-2018. Additionally, we include QGIS data mapping to visualize seasonal and regional differences across our dataset. We define our analysis across three following dimensions: 1) Presence of HABs, 2) High cyanobacteria levels: any cell counts ≥ 20,000 to 80,000/mL and 3) High cyanotoxin levels: any detected concentration ≥ 4 to 20 μg/L.
Results: Findings suggest cyanobacteria outbreaks mostly occur in the West North Central region of the US and during the summer months. US. Iowa, Vermont, Ohio, and North Carolina contain most of the reported outbreaks. Bloom occurrences similarly often occur during the summer but are mostly found in the New England area. Single factor ANOVA testing confirmed this result, finding at least one region to statistically differ in mean bloom count compared to other regions, significant at the 1% level. T- and Chi-sq tests all report significant differences in HAB status between regions and seasons as well. Chi-Sq results find a difference between bloom status and region at the 1% level. Two-sample T-tests (i.e., comparing each region vs. all other regions) find statistically significant differences with the East North Central (p<0.001), New England (p=0.019), Pacific (p=0.02), South Atlantic (p=0.006), and West North Central (p<0.001) regions. All seasons outside of Fall (p=0.112) are found to be statistically significantly different from all other times of the year at the 1% level. Finally, QGIS data mapping reiterates these regional and seasonal HAB and cyanobacterial differences in our dataset. The Midwest year-round and Western states Winter-Spring HAB exposure are definitively displayed in our figures, as well as New England’s Fall and Summer peak HAB concentrations.
Figure 1

Figure 2

Figure 3

Figure 4

Conclusion: Mitigating exposure to cyanobacterial toxicosis requires awareness of HAB regional and seasonal patterns. Our study finds HAB risks highest during the summer months, with regions following their own unique HAB seasonal patterns. We suggest government bodies incorporate these findings to better target their public awareness campaigns.
References
- Backer, Lorraine C., Deana Manassaram-Baptiste, Rebecca LePrell, and Birgit Bolton. “Cyanobacteria and algae blooms: review of health and environmental data from the harmful algal bloom-related illness surveillance system (HABISS) 2007–2011.” Toxins 7, no. 4 (2015): 1048-1064.
- Metcalf, J.S., Tischbein, M., Cox, P.A. and Stommel, E.W., 2021. Cyanotoxins and the nervous system. Toxins, 13(9), p.660.
- Rankin, K.A., Alroy, K.A., Kudela, R.M., Oates, S.C., Murray, M.J. and Miller, M.A., 2013. Treatment of cyanobacterial (microcystin) toxicosis using oral cholestyramine: case report of a dog from Montana. Toxins, 5(6), pp.1051-1063.
- Svirčev, Z., Lalić, D., Bojadžija Savić, G., Tokodi, N., Drobac Backović, D., Chen, L., Meriluoto, J. and Codd, G.A., 2019. Global geographical and historical overview of cyanotoxin distribution and cyanobacterial poisonings. Archives of toxicology, 93, pp.2429-2481.
- Trevino-Garrison, I., DeMent, J., Ahmed, F.S., Haines-Lieber, P., Langer, T., Ménager, H., Neff, J., Van der Merwe, D. and Carney, E., 2015. Human illnesses and animal deaths associated with freshwater harmful algal blooms—Kansas. Toxins, 7(2), pp.353-366.
- Zhang, F., Lee, J., Liang, S. and Shum, C.K., 2015. Cyanobacteria blooms and non-alcoholic liver disease: evidence from a county level ecological study in the United States. Environmental Health, 14(1), pp.1-11.
- “OHHABS Data | Harmful Algal Blooms (HABs).” Accessed: July 26, 2023. [Online]. Available: https://www.cdc.gov/habs/data/index.htm
Kidney Sales and Trafficking
Author Information1
Feng, Audrey2; Kovacs, Valerie3.; Lee, Crystal4; Peng, Kenneth5; Sajjad, Aryan6; Yeum, Daniel3.
(Editor: Wang, Zifu7)
1 All authors are listed in alphabetical order.
2 Green Hope High School, NC, 3 Thomas Jefferson High School for Science & Technology, VA, 4 Los Alamitos High School, CA, 5 Oakwood School, CA, 6 St. Paul VI Catholic High School, VA
7 George Mason University, VA
Background: Over the past few decades, international health authorities and law enforcement agencies have taken substantial initiatives to counteract the illicit practice of organ trade. These endeavors reflect a collective commitment to address the pressing issue of organ trafficking, which preys on vulnerable individuals and undermines ethical medical practices. In the 1980s and onwards, the World Health Organization (WHO) has been instrumental in formulating guidelines for human organ transplantation, emphasizing the importance of voluntary donations, transparency, and ethical sourcing [1]. Notably, INTERPOL launched Operation Organs in 2016, targeting criminal networks engaged in organ trafficking and emphasizing cross-border cooperation [4]. Despite the concerted efforts to combat the illegal practice of organ trade, instances of such illicit activities persist. The illicit kidney trade remains a complex and multifaceted phenomenon involving various transnational actors, including sellers, buyers, brokers, and surgical facilities [5]. A notable characteristic of this trade is the intricate network that often facilitates the transactions. For instance, affluent buyers typically do not directly engage with financially disadvantaged sellers. Instead, kidneys procured from economically marginalized individuals are often passed through intermediaries, commonly referred to as brokers [5]. Subsequently, medical facilities responsible for the surgical procedures are identified, contacted, and engaged by these buyers. While the complex interrelationships among agents spanning various countries have been acknowledged, there has yet to be a quantitative methodology explored to systematically detect and analyze the structure of these transnational networks engaged in organ trade. Typically, these networks are presented and examined on a case-by-case basis through individual reports, news articles, and various media channels. Given the inherent difficulty in eradicating these illicit transactions and their intricate multi-agent nature, it becomes imperative to explore the underlying network dynamics and establish a robust spatiotemporal database to comprehensively study these operations.
Objective: The study analyzed illegal kidney sales by generating a network of graphs using data of seller, buyer, and surgery countries and observed relationships among seller, buyer, and surgery countries.
Methods: Starting with an established dataset featuring information on kidney sellers’ and buyers’ nationalities, as well as surgery locations, the study entailed an in-depth examination of the kidney policies of each country under consideration. Data organization involved the meticulous arrangement of buyer, seller, surgery, and year information into a separate spreadsheet, ensuring its suitability for importation. The software Gephi was employed for crafting and analyzing network graphs. Specific network graphs were generated by importing data pairs, such as buyer and surgery records spanning particular years, to facilitate a more targeted analysis. Visualizations were optimized through adjustments to node and edge sizes, the removal of year labels to enhance clarity, and the utilization of the Fruchterman Reingold layout to improve the visualization of network connections.
Results: The network displays the count of Nodes and Edges for various years, illustrating both the countries involved and their connections. Additionally, it highlights the network’s diameter by showcasing the shortest path between the most distant nodes. Moreover, the network places emphasis on the central node, representing the most interconnected country, and provides insights into the average number of connections per country.
Figure 1. Network of Buyer, Sell, Surgery Countries
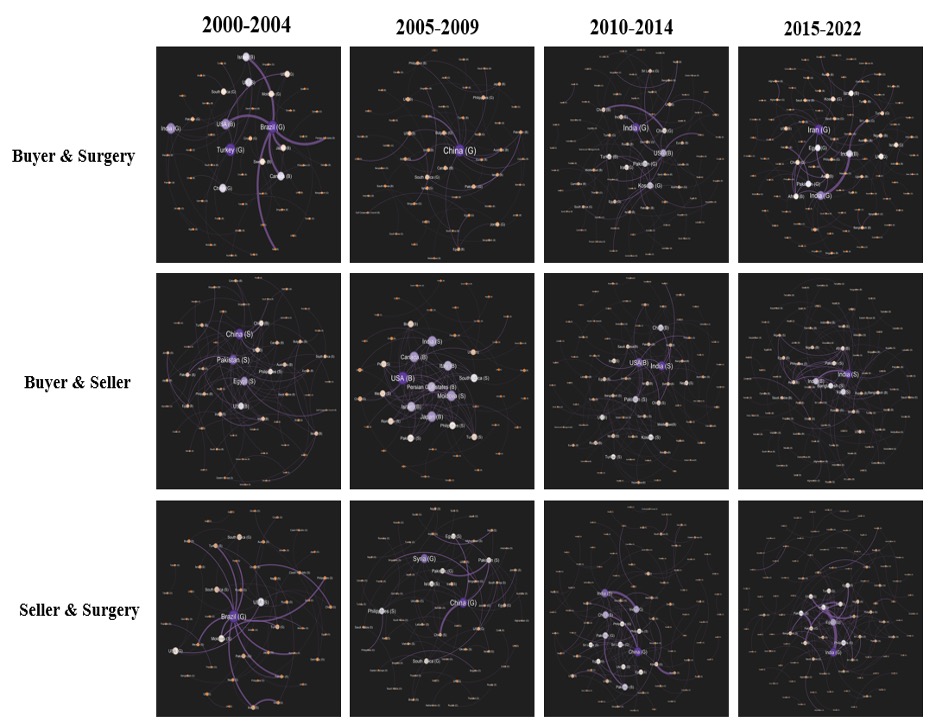
Conclusions: Our findings indicate that countries like the US and UK ranked highest in kidney sales. This suggests that nations with stronger economies tend to engage in more kidney purchases overall. Conversely, countries with weaker economies, such as India, Moldova, and the Philippines, often recorded higher kidney sales. In countries where kidney sales were legal, such as Brazil and China, certain patterns emerged in kidney surgeries. However, these trends shifted following policy changes and legal enforcement.
References
- World Health Organization. (2023). Transplantation. https://www.who.int/health-topics/transplantation#tab=tab_1
- The Transplantation Society. (2008). Declaration of Istanbul on Organ Trafficking and Transplant Tourism. https://www.declarationofistanbul.org/
- United Nations Office on Drugs and Crime. (2023). Global Database on Trafficking in Persons. https://www.unodc.org/human-trafficking/glotip.html
- INTERPOL. (2016). INTERPOL Operation Targeting Organized Crime Networks Behind Human Trafficking and Organ Trade. https://www.interpol.int/en/News-and-Events/News/2016/N2016-122
- 2017 Trafficking in Persons Report. https://www.state.gov/reports/2017-trafficking-in-persons-report
- Devlin, J., Chang, M.W., Lee, K. and Toutanova, K., 2018. Bert: Pre-training of deep bidirectional transformers for language understanding. arXiv preprint arXiv:1810.04805
- Touvron, H., Martin, L., Stone, K., Albert, P., Almahairi, A., Babaei, Y., Bashlykov, N., Batra, S., Bhargava, P., Bhosale, S. and Bikel, D., 2023. Llama 2: Open foundation and fine-tuned chat models. arXiv preprint arXiv:2307.09288.
Viruses and Host Membranes
Author Information1
Jacob, Riya2; Kefale, Mikael3; Khanna, Jahnavi4; Kim, Andrew Jacob5; McLaughlin, Madison6; Talwar, Ria7
(Editor: Li, Meng-Hao8)
1 All authors are listed in alphabetical order.
2 Briar Woods High School, VA; 3 Chantilly High School, VA; 4 McLean High School, VA, 5 Issaquah High School, CA; 6 John R. Lewis High School, VA; 7 Lakeside School, WA
8 George Mason University, VA
Background: Rabies is a zoonotic disease caused by an unsegmented RNA virus of the Lyssavirus genus. It spreads between animals and humans through contact with mucosal membranes, abrasions, or the saliva of an infected animal, most commonly a dog. The rabies virus travels through the body’s signal transmission pathways to reach the central nervous system and brain. Once it has entered the host, it attaches itself to nerve cells and begins to replicate. The virus then spreads throughout the body through neuronal pathways until it reaches the brain. The incubation period varies widely depending on the location of the bite and the severity of the infection. Once the virus reaches the brain, symptoms increase in severity, starting from flu-like symptoms to hydrophobia and delirium. The infected person enters the prodromal phase, during which they experience significant behavioral and physical changes, such as heightened aggression and pupil dilation. Progression to the “excited” or “furious” rabies phase leads to autonomic dysfunction and vicious, erratic behavior. The infected person may die in this phase or progress to the final stage, paralytic rabies, where they will eventually die [1][2][3].
Objective: This project aims to develop a comprehensive understanding of mechanisms for infectivity (attachment and entry) by defining the landscape of rabies virus research through bibliometrics analysis.
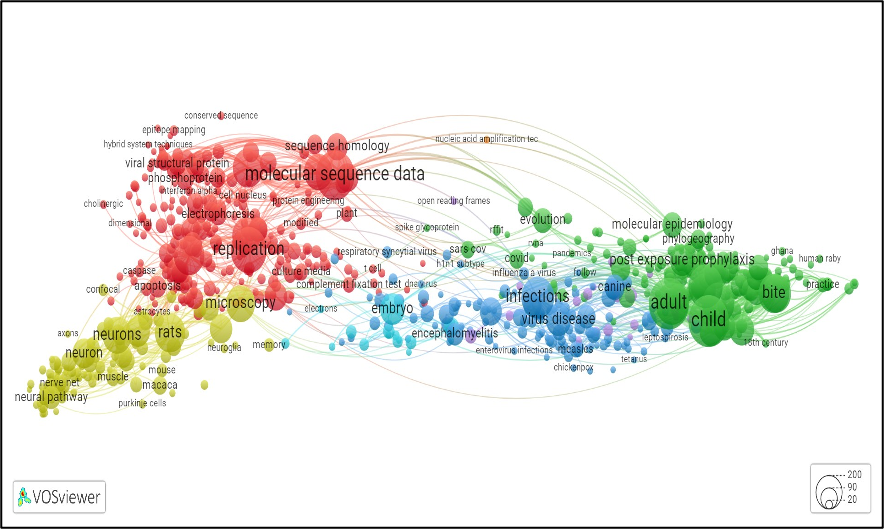
Methods: We obtained metadata related to the rabies virus from the PubMed database through the assistance of our GMU faculty advisors. This dataset encompasses keywords extracted from 8,589 articles published between 1993 and 2022. With guidance from our GMU faculty advisors, we utilized an R script to preprocess the data. This preprocessing involved eliminating articles with missing keywords and transforming the data from a long format to a wide format. Subsequently, we categorized the keywords into three distinct cohorts: 1993-2002, 2003-2012, and 2013-2022. Following data preparation, we conducted trend analysis by plotting the occurrences of keywords within these cohorts. We then transformed the data from its long format into an edge list, representing the co-occurrence of keywords within individual articles. This edge list served as the foundation for our network analysis, which aimed to uncover potential research directions within the field of rabies virus studies. For example, if one article featured keywords A and B, while another article featured keywords B and C, the co-occurrence of keywords A and C hinted at potential research avenues. In the final stages of our analysis, we visualized the networks depicting keyword associations. This visualization allowed us to explore and assess promising research directions within the realm of rabies virus research.
Results: First, an article’s keywords serve as indicators of the central and significant topic addressed in the research articles. Our results illustrated that the predominant research emphasis has revolved around antibodies and phylogeny, and this trend is expected to persist due to the absence of a developed vaccine for advanced stages of Rabies. Notably, the first and second cohorts’ top 10 keywords include the term “antigen,” whereas the third cohort omits it. This implies that antigens have ceased to be a prominent area of focus within Rabies research. Second, the analytical results illustrated that the term “proteins” often relates to infectivity, implying their significant influence on virus attachment and cell entry, ultimately resulting in harm. The rabies virus supports this concept by modifying its envelope proteins to adhere to host cell receptors. It is vital to reinforce host cell receptors to prevent harmful proteins from penetrating. Moreover, studies on the impacts of the rabies virus have broadened to encompass various behaviors such as feeding, homing, sexual activity, and cooperation, in addition to aggression. Finally, the network analysis illustrates the most pertinent terms linked to the rabies virus from 1993 to 2023. The lines that connect these words demonstrate that many articles contain various relevant keywords. Words that are not connected could lead to potential research questions. Some words have larger bubbles because they appear more frequently alongside other relevant words in articles. For example, “molecular sequence data” is notable, appearing 511 times in relation to other words, while “leptospirosis” is less frequent, with only 16 occurrences.
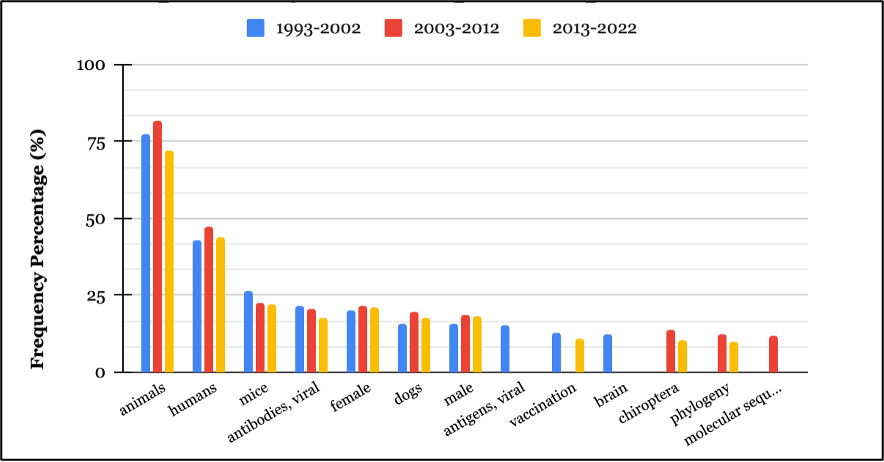
Conclusions: Over time, there has been a noticeable increase in both novel research questions and research approaches in rabies virus studies. Notably, proteins are known to play a crucial role in virus attachment and entry. Also, the trends suggest a discernible rise in specialized research areas, particularly in the domain of behavioral studies.
References
- Yousaf, M.Z., Qasim, M., Zia, S., Rehman Khan, M.U., Ashfaq, U.A. and Khan, S., 2012. Rabies molecular virology, diagnosis, prevention and treatment. Virology journal, 9, pp.1-5.
- Rabies Exposure in Healthcare Settings. (2021). Centers for Disease Control and Prevention. https://www.cdc.gov/rabies/specific_groups/hcp/exposure.html
- How is rabies transmitted? (2019). Centers for Disease Control and Prevention. https://www.cdc.gov/rabies/transmission/index.html